Cyclosporine
Isolated from a soil fungus, cyclosporine is a cyclic peptide immunosuppressant that dampens the immune response by inhibiting calcineurin. Blocking this enzyme prevents T cells from producing interleukin-2, the signal that drives their activation and proliferation, which is why the drug is central to preventing rejection of transplanted organs. The same T-cell restraint makes it valuable in autoimmune conditions such as psoriasis, rheumatoid arthritis, and Crohn's disease. A large molecule (C62H111N11O12, molecular weight above 1,200) classified as a protein-type agent, it has a half-life of about 6 to 12 hours. Its selectivity for the T-cell activation pathway allows targeted immune suppression, though careful management of drug levels accompanies its use. Cyclosporine is an approved cornerstone of transplant medicine.
A calcineurin inhibitor immunosuppressant derived from a fungus that selectively suppresses T-cell activity by blocking interleukin-2 production, essential for preventing organ transplant rejection. It is also used for autoimmune conditions including psoriasis, rheumatoid arthritis, and Crohn's disease.
分子量
1202.6100 g/mol
LogP
7.50
TPSA
279.00 Ų
リピンスキーの五則
不適合
治療領域
薬物分類
作用機序
Calcineurin inhibitor suppressing T-cell activation.
Pharmacokinetics (PK)
Pharmacodynamics (PD)
Calcineurin inhibitor suppressing T-cell activation.
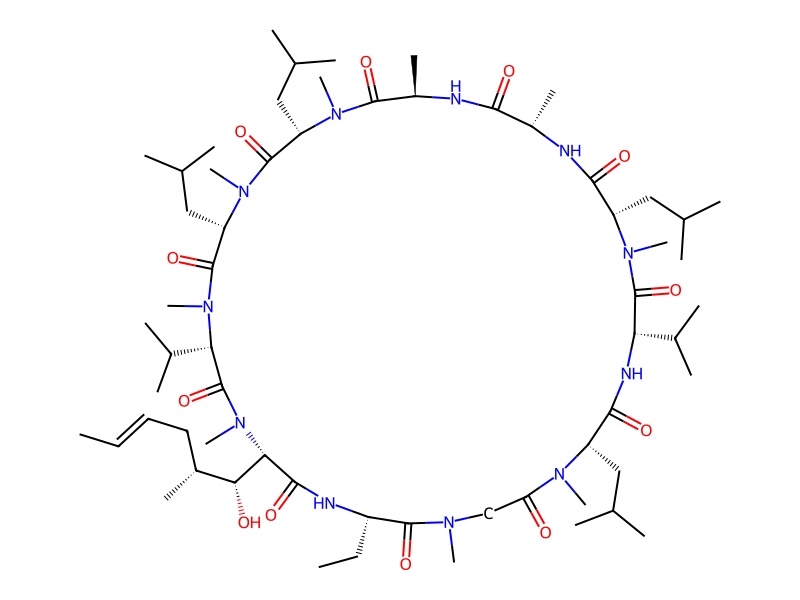
2D構造
{kind=link}
{kind=link}
Cite this structure
Embed this structure
SMILES
C/C=C/C[C@@H](C)[C@@H](O)[C@H]1C(=O)N[C@@H](CC)C(=O)N(C)CC(=O)N(C)[C@@H](CC(C)C)C(=O)N[C@@H](C(C)C)C(=O)N(C)[C@@H](CC(C)C)C(=O)N[C@@H](C)C(=O)N[C@H](C)C(=O)N(C)[C@@H](CC(C)C)C(=O)N(C)[C@@H](CC(C)C)C(=O)N(C)[C@@H](C(C)C)C(=O)N1C
InChI
InChI=1S/C62H111N11O12/c1-25-27-28-40(15)52(75)51-56(79)65-43(26-2)58(81)67(18)33-48(74)68(19)44(29-34(3)4)55(78)66-49(38(11)12)61(84)69(20)45(30-35(5)6)54(77)63-41(16)53(76)64-42(17)57(80)70(21)46(31-36(7)8)59(82)71(22)47(32-37(9)10)60(83)72(23)50(39(13)14)62(85)73(51)24/h25,27,34-47,49-52,75H,26,28-33H2,1-24H3,(H,63,77)(H,64,76)(H,65,79)(H,66,78)/b27-25+/t40-,41+,42-,43+,44+,45+,46+,47+,49+,50+,51+,52-/m1/s1
Molecular Formula
C62H111N11O12
HBD / HBA
5 / 12
回転可能結合数
15
重原子数
85
Cyclosporine, a strong dual inhibitor of CYP3A4 and P-glycoprotein, substantially increases rivaroxaban exposure and bleeding risk.
Cyclosporine dramatically increases dabigatran exposure through P-gp inhibition, raising the risk of serious or life-threatening bleeding.
Cyclosporine raises simvastatin exposure by 6- to 10-fold through inhibition of CYP3A4, OATP1B1, and P-gp, creating an extremely high risk of rhabdomyolysis.
Concurrent use of cyclosporine and tacrolimus dramatically amplifies nephrotoxicity and is generally contraindicated; both agents independently cause renal vasoconstriction and tubular injury.
Methylprednisolone inhibits CYP3A4-mediated cyclosporine metabolism, raising cyclosporine levels; conversely, cyclosporine may increase methylprednisolone exposure — a bidirectional pharmacokinetic interaction.
Cyclosporine inhibits OATP1B1/1B3 hepatic transporters and P-glycoprotein, substantially increasing pravastatin plasma concentrations and raising the risk of myopathy and rhabdomyolysis.
Cyclosporine significantly increases apixaban exposure through inhibition of CYP3A4 and P-glycoprotein, elevating bleeding risk.
Cyclosporine dramatically increases atorvastatin plasma levels through combined inhibition of CYP3A4, OATP1B1, and P-gp, substantially raising the risk of myopathy and rhabdomyolysis.
Carbamazepine dramatically reduces cyclosporine plasma levels through potent CYP3A4 induction, placing transplant patients at severe rejection risk.
Cyclosporine inhibits CYP3A4-mediated amlodipine metabolism, increasing amlodipine plasma concentrations and the risk of pronounced vasodilation and peripheral edema.
Concurrent use of acyclovir and cyclosporine can increase nephrotoxicity risk, as both agents are renally cleared and individually nephrotoxic.
Combining adalimumab with cyclosporine produces substantial additive immunosuppression, increasing the risk of serious opportunistic infections, lymphoma, and other immunosuppression-related malignancies.
No side effects recorded
Side effect data is not yet available for this drug.
よくある質問
A calcineurin inhibitor immunosuppressant derived from a fungus that selectively suppresses T-cell activity by blocking interleukin-2 production, essential for preventing organ transplant rejection. It is also used for autoimmune conditions including psoriasis, rheumatoid arthritis, and Crohn's disease.
Calcineurin inhibitor suppressing T-cell activation.
Key pharmacokinetic parameters for Cyclosporine: Half-life: 6-12 hours.
Yes, Cyclosporine is an approved drug. It has reached clinical phase 4. It is classified as a Protein.
Related Drugs
Same Drug Class
References & Data Sources
- ChEMBL — European Bioinformatics Institute (EBI). CHEMBL160. Open-access bioactivity database.
- PubChem — National Center for Biotechnology Information (NCBI). CID 5284373. Chemical information database.
Data aggregated from publicly available pharmacological databases. Last updated 2026-03-04.
Embed This Widget
Add the script tag and a data attribute to embed this widget.
<script src="https://cdn.jsdelivr.net/npm/drugfyi-embed@1/dist/embed.min.js" defer></script>
<div data-drugfyi="drug" data-slug="cyclosporine"></div>Embed via iframe for maximum compatibility.
<iframe src="https://drugfyi.com/iframe/drug/cyclosporine/" width="420" height="400" frameborder="0" style="border:0;border-radius:10px;max-width:100%" loading="lazy"></iframe>Paste this URL in WordPress, Medium, or any oEmbed-compatible platform.
https://drugfyi.com/drug/cyclosporine/Add a dynamic SVG badge to your README or docs.
[](https://drugfyi.com/drug/cyclosporine/)Use the native HTML custom element.
<script src="https://cdn.jsdelivr.net/npm/drugfyi-embed@1/dist/embed.min.js" defer></script>
<drugfyi-drug slug="cyclosporine"></drugfyi-drug>