Aspirin
Among the oldest medicines still in everyday use, aspirin irreversibly inhibits the cyclooxygenase enzymes COX-1 and COX-2, cutting the production of prostaglandins that generate pain, fever, and inflammation. The irreversibility of that block is what sets it apart: in platelets, which cannot make new enzyme, a single low dose suppresses clot-promoting thromboxane for the cell's lifetime. This dual character explains why higher doses relieve pain and fever while low doses are taken to lower the risk of heart attack and stroke. A small molecule (C9H8O4) with a parent half-life of only 2 to 3 hours, aspirin is rapidly converted to salicylate after absorption. It remains an approved, globally stocked drug whose antiplatelet role reshaped cardiovascular prevention.
One of the oldest and most widely used medicines, aspirin irreversibly inhibits cyclooxygenase enzymes, reducing the production of prostaglandins that cause pain, fever, and inflammation. At low doses it prevents platelets from clumping together, making it valuable for reducing the risk of heart attack and stroke.
Moleküler Ağırlık
180,1580 g/mol
LogP
1,20
TPSA
63,60 Ų
Lipinski RO5
Geçer
Terapötik Alanlar
İlaç Sınıfları
Etki Mekanizması
Irreversibly inhibits cyclooxygenase-1 and -2.
Pharmacokinetics (PK)
Pharmacodynamics (PD)
Irreversibly inhibits cyclooxygenase-1 and -2.
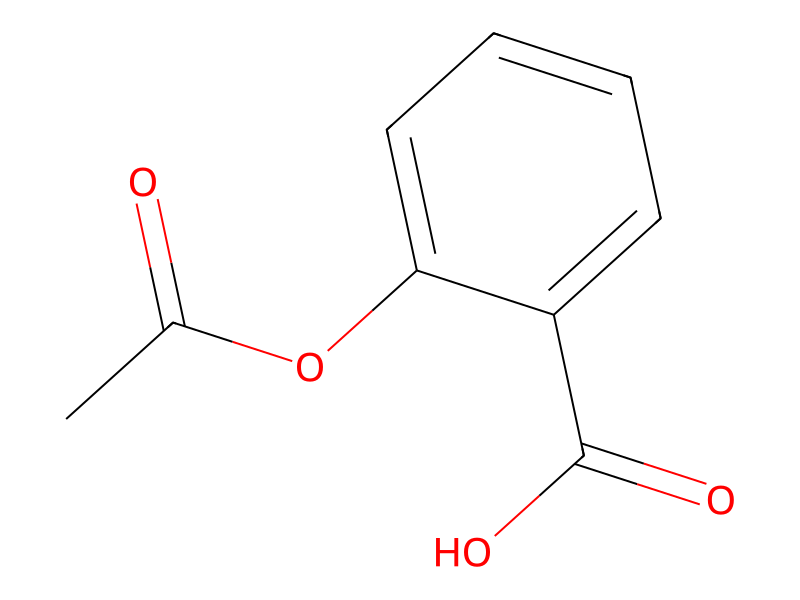
2D Yapı
{kind=link}
{kind=link}
Cite this structure
Embed this structure
SMILES
CC(=O)Oc1ccccc1C(=O)O
InChI
InChI=1S/C9H8O4/c1-6(10)13-8-5-3-2-4-7(8)9(11)12/h2-5H,1H3,(H,11,12)
Molecular Formula
C9H8O4
HBD / HBA
1 / 4
Döndürülebilir Bağlar
3
Ağır Atomlar
13
Aspirin reduces methotrexate clearance by competing for renal tubular secretion, raising plasma methotrexate levels and toxicity risk.
Concurrent use significantly increases bleeding risk through dual anticoagulant/antiplatelet mechanisms. Even low-dose aspirin (81 mg) meaningfully raises the risk of major hemorrhage.
Diphenhydramine may modestly reduce aspirin absorption and slightly impair its antiplatelet efficacy through delayed gastric emptying; the clinical significance is generally low.
Combining aspirin with celecoxib provides no additional gastroprotective benefit over aspirin alone and may negate the GI advantage of celecoxib, increasing the risk of mucosal injury.
Adding aspirin to rivaroxaban increases bleeding risk through additive antithrombotic effects; some indications (COMPASS trial) use this combination with careful patient selection.
Aspirin combined with fluoxetine increases GI hemorrhage risk through synergistic platelet impairment and CYP2C9-mediated interactions.
Prednisone may increase salicylate clearance, reducing aspirin's anti-inflammatory efficacy, and combined GI toxicity is substantially increased.
Low-dose aspirin combined with dabigatran increases bleeding risk; clinical evidence suggests a 2-fold increase in major bleeding events.
The combination of aspirin and sertraline increases upper GI bleeding risk through synergistic antiplatelet and platelet serotonin depletion effects.
Ibuprofen can block aspirin's irreversible platelet inhibition by competing for the same COX-1 active site, potentially reducing aspirin's cardioprotective effect.
Dual antiplatelet therapy with aspirin and clopidogrel provides superior thrombotic protection post-ACS and post-PCI but approximately doubles the risk of major bleeding compared with aspirin alone.
Combining aspirin with escitalopram increases the risk of GI bleeding through additive impairment of hemostasis.
Low-dose aspirin reduces the uricosuric effect of allopurinol and may increase uric acid levels, potentially triggering gout flares.
Combining apixaban with aspirin increases major bleeding risk beyond that of either agent alone through additive antithrombotic and gastric mucosal effects.
No side effects recorded
Side effect data is not yet available for this drug.
Sıkça Sorulan Sorular
One of the oldest and most widely used medicines, aspirin irreversibly inhibits cyclooxygenase enzymes, reducing the production of prostaglandins that cause pain, fever, and inflammation. At low doses it prevents platelets from clumping together, making it valuable for reducing the risk of heart attack and stroke.
Irreversibly inhibits cyclooxygenase-1 and -2.
Key pharmacokinetic parameters for Aspirin: Half-life: 2-3 hours.
Yes, Aspirin is an approved drug. It has reached clinical phase 4. It is classified as a Small molecule.
Related Drugs
Same Drug Class
References & Data Sources
- ChEMBL — European Bioinformatics Institute (EBI). CHEMBL25. Open-access bioactivity database.
- PubChem — National Center for Biotechnology Information (NCBI). CID 2244. Chemical information database.
Data aggregated from publicly available pharmacological databases. Last updated 2026-03-04.
Embed This Widget
Add the script tag and a data attribute to embed this widget.
<script src="https://cdn.jsdelivr.net/npm/drugfyi-embed@1/dist/embed.min.js" defer></script>
<div data-drugfyi="drug" data-slug="aspirin"></div>Embed via iframe for maximum compatibility.
<iframe src="https://drugfyi.com/iframe/drug/aspirin/" width="420" height="400" frameborder="0" style="border:0;border-radius:10px;max-width:100%" loading="lazy"></iframe>Paste this URL in WordPress, Medium, or any oEmbed-compatible platform.
https://drugfyi.com/drug/aspirin/Add a dynamic SVG badge to your README or docs.
[](https://drugfyi.com/drug/aspirin/)Use the native HTML custom element.
<script src="https://cdn.jsdelivr.net/npm/drugfyi-embed@1/dist/embed.min.js" defer></script>
<drugfyi-drug slug="aspirin"></drugfyi-drug>