Warfarin
Warfarin is an oral anticoagulant that interferes with the vitamin K cycle by inhibiting the vitamin K epoxide reductase complex. Suppressing this enzyme lowers the liver's output of vitamin K-dependent clotting factors and slows the coagulation cascade. The resulting effect makes it useful for preventing and treating blood clots, including deep vein thrombosis and pulmonary embolism, and for reducing stroke risk in atrial fibrillation and in recipients of mechanical heart valves. Because the response develops over several days and shifts with diet, other medicines, and supplements, therapy is titrated against the INR blood test to hold anticoagulation within a target range. A small synthetic molecule (C19H16O4) with an elimination half-life of roughly 20 to 60 hours, warfarin has remained one of the most widely used anticoagulants for decades despite its many interactions.
This anticoagulant (blood thinner) medication is used to prevent and treat blood clots, including those in deep veins (DVT), the lungs (pulmonary embolism), and to reduce the risk of stroke in patients with atrial fibrillation or artificial heart valves. It works by blocking the production of vitamin K-dependent clotting factors in the liver. It requires frequent blood tests (INR monitoring) to keep the dose in a safe and effective range, and interacts with many foods, medications, and supplements.
Khối lượng phân tử
308,3280 g/mol
LogP
2,70
TPSA
63,60 Ų
Lipinski RO5
Đạt
Lĩnh vực điều trị
Phân loại thuốc
Cơ chế tác dụng
Inhibits vitamin K epoxide reductase complex.
Pharmacokinetics (PK)
Pharmacodynamics (PD)
Inhibits vitamin K epoxide reductase complex.
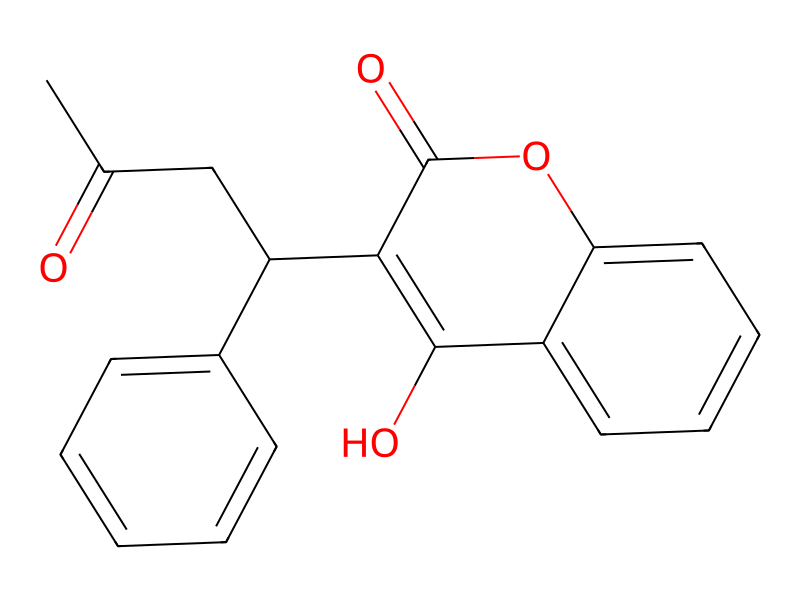
Cấu trúc 2D
{kind=link}
{kind=link}
Cite this structure
Embed this structure
SMILES
CC(=O)CC(c1ccccc1)c1c(O)c2ccccc2oc1=O
InChI
InChI=1S/C19H16O4/c1-12(20)11-15(13-7-3-2-4-8-13)17-18(21)14-9-5-6-10-16(14)23-19(17)22/h2-10,15,21H,11H2,1H3
Molecular Formula
C19H16O4
HBD / HBA
1 / 4
Liên kết có thể quay
4
Nguyên tử nặng
23
Zolpidem has been reported to modestly increase warfarin anticoagulation in isolated case reports; routine clinical concern is low.
Methotrexate combined with warfarin increases bleeding risk and may cause enhanced anticoagulation; both drugs share protein-binding sites, amplifying free drug concentrations.
Phenytoin and warfarin have a complex bidirectional interaction: phenytoin initially inhibits warfarin metabolism (raising INR) but then induces it (lowering INR), making anticoagulation management unpredictable.
Fluconazole dramatically increases warfarin exposure, causing large INR elevations and a high risk of serious or life-threatening bleeding.
Naproxen combined with warfarin increases the risk of GI and other hemorrhagic complications through additive effects on hemostasis and direct gastric mucosal damage.
Tamoxifen dramatically increases warfarin anticoagulation, causing large INR elevations and a substantially elevated risk of serious bleeding.
Carbamazepine markedly reduces warfarin plasma concentrations, potentially resulting in sub-therapeutic anticoagulation and increased thromboembolic risk.
Ibuprofen combined with warfarin substantially increases bleeding risk, particularly gastrointestinal hemorrhage, through complementary antiplatelet and mucosal injury mechanisms.
Concurrent use significantly increases bleeding risk through dual anticoagulant/antiplatelet mechanisms. Even low-dose aspirin (81 mg) meaningfully raises the risk of major hemorrhage.
Metronidazole markedly potentiates warfarin anticoagulation, leading to supratherapeutic INR levels and an elevated risk of serious bleeding.
Omeprazole may modestly increase warfarin plasma concentrations through weak CYP2C19 inhibition; the clinical effect is generally small but warrants awareness.
Amoxicillin may slightly potentiate warfarin by reducing gut flora that synthesize vitamin K2, though the effect is generally small and inconsistent.
Oseltamivir does not appear to meaningfully alter warfarin pharmacokinetics; however, the febrile illness being treated may independently elevate INR, which can be mistakenly attributed to the antiviral.
Ranitidine can modestly increase warfarin plasma levels and INR by inhibiting CYP2C9-mediated warfarin metabolism, though the magnitude is smaller than with cimetidine.
Cephalexin may enhance the anticoagulant effect of warfarin, with case reports describing INR elevation during concurrent therapy, likely through disruption of vitamin K-producing gut flora.
Clindamycin may enhance the anticoagulant effect of warfarin by disrupting vitamin K-producing gut flora, leading to unpredictable INR elevations and increased bleeding risk during and shortly after the antibiotic course.
Trimethoprim (alone or in combination as TMP-SMX) increases warfarin's anticoagulant effect through CYP2C9 inhibition, raising INR and bleeding risk.
Hydroxychloroquine may potentiate the anticoagulant effect of warfarin, raising INR and the risk of bleeding complications.
Colchicine may increase bleeding risk when combined with warfarin; isolated case reports suggest possible INR elevation, though the mechanism is not well characterized.
Regular or high-dose acetaminophen can potentiate the anticoagulant effect of warfarin, leading to INR elevation and increased bleeding risk, even though single analgesic doses carry a lower risk.
Semaglutide slows gastric emptying, potentially reducing and delaying oral warfarin absorption, leading to variable changes in INR that complicate anticoagulation management.
Simvastatin modestly potentiates warfarin anticoagulation, leading to small but potentially clinically relevant INR increases.
Levothyroxine enhances the catabolism of vitamin K-dependent clotting factors, amplifying warfarin's anticoagulant effect and raising the risk of bleeding when thyroid replacement is initiated or doses are increased.
Azithromycin can potentiate the anticoagulant effect of warfarin, leading to elevated INR and increased bleeding risk during and shortly after the antibiotic course.
Sertraline can modestly increase warfarin anticoagulation through weak CYP2C9 inhibition combined with SSRI-mediated platelet serotonin depletion.
Fluoxetine increases warfarin plasma levels via CYP2C9 inhibition and may independently impair platelet function, raising hemorrhagic risk.
Corticosteroids have a complex and variable interaction with warfarin; high doses may increase bleeding risk via GI mucosal effects while also affecting clotting factor synthesis.
Rosuvastatin increases warfarin plasma concentrations through inhibition of CYP2C9, potentially leading to supratherapeutic INR values.
Ciprofloxacin consistently enhances warfarin's anticoagulant effect, raising INR and increasing the risk of bleeding complications.
Doxycycline may enhance warfarin's anticoagulant effect, particularly in patients whose vitamin K intake is already limited.
Celecoxib, a selective COX-2 inhibitor, can inhibit CYP2C9-mediated warfarin metabolism and may increase GI bleeding risk, though platelet function is less impaired than with non-selective NSAIDs.
Valproic acid can displace warfarin from plasma protein binding sites and may inhibit platelet aggregation, increasing bleeding risk.
No side effects recorded
Side effect data is not yet available for this drug.
Câu hỏi thường gặp
This anticoagulant (blood thinner) medication is used to prevent and treat blood clots, including those in deep veins (DVT), the lungs (pulmonary embolism), and to reduce the risk of stroke in patients with atrial fibrillation or artificial heart valves. It works by blocking the production of vitamin K-dependent clotting factors in the liver. It requires frequent blood tests (INR monitoring) to keep the dose in a safe and effective range, and interacts with many foods, medications, and supplements.
Inhibits vitamin K epoxide reductase complex.
Key pharmacokinetic parameters for Warfarin: Half-life: 20-60 hours.
Yes, Warfarin is an approved drug. It has reached clinical phase 4. It is classified as a Small molecule.
Related Drugs
References & Data Sources
- ChEMBL — European Bioinformatics Institute (EBI). CHEMBL1464. Open-access bioactivity database.
- PubChem — National Center for Biotechnology Information (NCBI). CID 54678486. Chemical information database.
Data aggregated from publicly available pharmacological databases. Last updated 2026-03-28.
Embed This Widget
Add the script tag and a data attribute to embed this widget.
<script src="https://cdn.jsdelivr.net/npm/drugfyi-embed@1/dist/embed.min.js" defer></script>
<div data-drugfyi="drug" data-slug="warfarin"></div>Embed via iframe for maximum compatibility.
<iframe src="https://drugfyi.com/iframe/drug/warfarin/" width="420" height="400" frameborder="0" style="border:0;border-radius:10px;max-width:100%" loading="lazy"></iframe>Paste this URL in WordPress, Medium, or any oEmbed-compatible platform.
https://drugfyi.com/drug/warfarin/Add a dynamic SVG badge to your README or docs.
[](https://drugfyi.com/drug/warfarin/)Use the native HTML custom element.
<script src="https://cdn.jsdelivr.net/npm/drugfyi-embed@1/dist/embed.min.js" defer></script>
<drugfyi-drug slug="warfarin"></drugfyi-drug>